Diathermy.
List of contents.
-
introduction
-
suggested reading
-
basic information
and "buzz" words
-
electricity
-
diathermy
-
voltage
-
current
-
resistance
-
conductor
-
resistor
-
capacitor
-
direct current
-
alternating current
-
expanded
information
-
what is diathermy?
-
types of diathermy
-
unipolar
-
bipolar
-
uses of diathermy current
-
cutting
-
coagulating
-
blended: a mix of cutting and coagulating
-
fulgurating
-
problems with
diathermy
-
bipolar
-
unipolar
-
direct coupling
-
capacitive coupling
-
suggested model for
a MRCOG viva station
Introduction.
This subject has come up as a viva in the
OSCE exam.
How would you feel if asked to discourse on
the subject for 15 minutes without prompting?
The following gives you what you need to
know.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Suggested reading.
There is good coverage in
"Basic
Practical Skills in Obstetrics and Gynaecology",
published by the RCOG Press.
And a detailed education module by
Valley Lab
that is worth going through to get a solid grounding.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Buzz
words:
Electricity:
For our purposes it is the flow of electrons through a conductor, e.g. a
metal.
The electrons hop from one atom to the
next.
Something has to drive them along.
This could be a battery, a generator like
a diathermy machine or various electric and magnetic fields.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Diathermy:
Diathermy means the use of electricity to generate heat.
In surgery it is used
:
to vaporise tissue
for cutting purposes,
or to coagulate it to effect haemostasis or destroy tissue.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Voltage.
This is the force making the electrons
move.
The word is a tribute to
Alessandro Volta,
one of the pioneers in the field.
Use an ordinary AA battery and you shove the electrons with 1.5 volts.
Use two batteries, in series, i.e. one behind the other, and you get 3 volts.
The greater the voltage, the more
electrons flow, so the greater the current.
Put one finger on the top of an AA battery and one on the bottom.
You now have 1.5 volts applied across
your fingers.
The resistance to current flowing through your body is so great that very little
electricity flows and you feel nothing.
But put your fingers in the socket of the ring main and you will probably kill
yourself.
The voltage of the ring main is 250 and a significant amount of current will
flow.
With high voltages electrons can jump
gaps in air, as in fulguration below.
Higher voltages increase the risk of
capacitive coupling. See below.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Current:
this is the amount of electricity that is flowing.
it is the number of electrons flying past a fixed point per second.
The basic unit is the "ampere".
Named after Andre Marie Ampere
about
whom you can read more here.
Though why you would want to do so I do
not know.
Electricity generates heat in the
material it is going through.
The amount of heat is determined by the
formula: heat = I 2 x R.
"I" is the current and
"R" is the resistance to the passage of electricity of the material it
is flowing through.
So the amount of current is really
important.
A standard electric bulb has a metal filament that heats up as the electricity
flows through it.
For
our purposes it has a fixed resistance.
Plug
a 12 volt bulb into the mains (240 volts) and it will become extremely bright
for an instant then blow.
The force driving the electrons is 20 times greater than the bulb is designed for.
So
the current is 20 times greater than it should be.
The
amount of heat generated will be 400 times greater than the design
limits.
The
filament will overheat, generating a bright flash, then melt.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Resistance: This
is the amount of difficulty a material presents to the flow of electricity.
Most metals have low resistance, so electricity flows
easily through them.
Plastic and rubber usually have high resistance.
The wire that goes to your table lamp has a copper core, to let current flow
freely.
It has a plastic covering, so that you don't get electrocuted if you touch it.
go to the top of the
page
go to the
list of contents
go to the bottom of the page and
other links
Conductor
: a
material that allows electrons to flow through it.
Copper is commonly used for electric
wires as it has low resistance.
go to the top of the
page
go to the list of
contents
go to the bottom of the page and
other links
Resistor:
a material that is highly resistant to the flow of electrons.
Everything has some degree of resistance.
The exception being
super-conductors which, theoretically, can have zero resistance.
But you need to cool them to close to
absolute zero.
This is -273O Celsius, so not
something you can achieve in your fridge or freezer.
But you can put huge currents through
them without generating much heat.
Heat = I 2 x R.
If R = 0, then I 2 x R = 0
and no heat is generated.
This is useful for creating huge magnetic
fields such as are used in MRI
.
Interesting, but of no relevance to diathermy & the MRCOG.
go to the top of the
page
go to the list of
contents
go to the bottom of the page and
other links
Capacitor:
this is an electrical device made up of two conductors separated by a
resistor.
Diagrammatically it is:

The two ovals are meant to represent two metal discs with wires attached.
In this case they are separated by air.
So, you have two conductors (the metal plates) separated by a resistor (air).
Capacitors have a remarkable feature.
A
current flowing in one of the discs and attached wire can induce a current in
the opposite disc and wire.
The
peculiarity is that the induced current occurs although there is no contact
between the discs/ wires on the two sides.
This
is the basis of the ill-understood capacitive coupling.
When you operate diathermy equipment, current flows through the instrument you
use and its connection leads.
This
current can induce current in adjacent metal objects, or even tissues, without
direct contact.
The
induced current could create enough heat to damage tissue.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Direct
current: this is electricity that flows in one direction only.
It is not used in diathermy.
It used to be used in cautery.
A current was passed through a wire, heating it.
The hot wire could then be used to cut or destroy tissues.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Alternating
current:
this is electricity that alternately flows one way and then the other.
The
Grand Old Duke of York of electricity.
Household
electricity is alternating current.
The
frequency of the changes in direction of flow is 50 cycles per second.
Diathermy
uses vastly higher frequencies.
The
unit of frequency is the Hertz.
1
Hz = 1 cycle per second.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Expanded information about diathermy.
Diathermy:
this is the use of electricity to generate heat in tissues.
For the surgeon, the heating has to be
enough to vaporize or coagulate the tissue.
The electricity has to be of high frequency, usually referred to as
radio-frequency.
This
is because it falls into the range of
frequencies used for wireless transmissions.
One
of the main values of the high frequency is that it is too fast to stimulate
nerve fibres.
This
means that you do not get spasm or paralysis of muscle.
To avoid these unwanted effects, you need
frequencies greater than 100 kHz.
Diathermy units use frequencies from 500
kHz (500,000 cycles per second) to 2 MHz (2 million cycles per second).
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Types of diathermy
There are two types used in
surgery: unipolar and bipolar.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Unipolar:
this is the type of diathermy that is most often used in surgery,
including open, minimally invasive, colposcopic and hysteroscopic.
It is like the simple circuits you may
have created as a child.

Electrons are driven by the battery up from the negative terminal,
through the bulb, making it light up.
They go back through the +ve terminal and
through the battery.
This is a circuit.
The same applies to a patient.
You have to create a circuit for the
current to flow round.
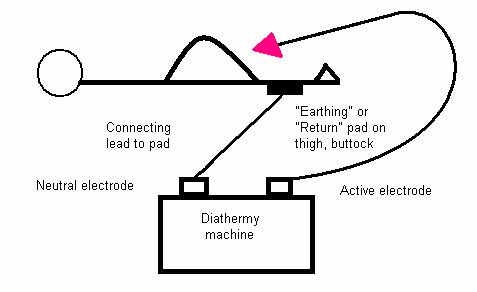
Follow the wire from the active electrode on the diathermy machine.
It goes to the device (needle point,
scissors, forceps etc.) you will use to apply the diathermy to the patient.
Once the device is applied to the
patient, the current will flow from the point of contact.
It will spread out as it passes through
the patient, heading for the return pad, which is usually attached to the
patient’s thigh.
From there it runs back to the diathermy
machine, so completing the circuit.
Tissues will be heated according to the
amount of electric current running through them. Remember heat = I 2 x
R.
The greatest current per cubic centimetre
of tissue will be at the point of contact of the active electrode.
The tissue in this area will usually be
coagulated or vaporised.
Away from the immediate point of contact
of the active electrode, the current spreads out.
So the amount going through any cubic
centimetre will be small and the temperature rise will be insufficient to cause
tissue damage.
The return pad must be applied over a
large area.
This ensures that the return current is
spread out.
It cannot cause burns under the pad as
the current flow per square centimetre of skin will be small.
Modern machines test to ensure that the
pad is properly applied.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Bipolar:
this is a very safe form of diathermy.
Usually you use forceps.
The current only flows between the tips
of the forceps, from the active electrode to the neutral electrode.
So there is less risk of stray currents
damaging tissues other that those you are aiming to damage.

go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Uses
of diathermy current.
There are three
main types: cutting, coagulating, and blended.
Cutting
current.
Key data for the exam: continuous
current at low voltage: 500 to 1,000 volts.
The water in the cells is
turned to steam, so the cells vaporise giving a cutting effect.
The best effect will occur
when the current flows through the smallest tissue volume.
Obviously, using a clean
needle point will produce this.
The current flows
continuously.
In other modalities, the current is applied in bursts.
You are only vaporising the
tissue in the immediate vicinity of the needle.
So you do not need a high
voltage to drive significant current into deep layers.
So, for MCQs and even the
dreaded OSCE viva, this is continuous current but relatively low voltage (500
to 1000 volts).
Because the effect is
relatively superficial and the tissues are vaporised, not coagulated, there is
no great haemostasis.
This is used in
laparoscopic surgery for dividing adhesions, myomectomy etc.
The total tissue damage is
less, so smoke production is less.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Coagulating
current.
Key data: bursts of
current at high voltage: up to 6,000 volts.
The aim of this is to
desiccate the tissue, but not to vaporise it.
You want to generate lower
tissue temperatures than with cutting current.
This is done by applying
the current in bursts.
Usually it is applied for
< 10% of the time the pedal is operated.
You are treating bigger
volumes of tissue and want the effect to go deeper than with cutting.
So a higher voltage is
used, usually up to 6,000 volts.
Coagulating current
provides good haemostasis.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Blended
current.
Key data. Intermediate
voltage and duration of current.
This cuts and coagulates.
Current is applied for up
to 50% of the time and at voltages of up to 2,000.
This means slower cutting
than the continuous pure cutting current, but provides coagulation as well.
A typical use would be loop
excision of CIN.
The cutting current gives
the wire the ability to excise tissue; the coagulating current provides
haemostasis.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Fulguration.
This is not much used in
gynaecology.
It is like a scatter-gun
to blast a wide area.
The active electrode is
kept at a distance from the tissue to be treated.
So the electricity has to
pass through air (or CO2 at laparoscopy).
Air and CO2 have high resistance, so
high voltage is needed to drive the current.
The high voltage creates an
electrical arc, like a mini lightning bolt, between the electrode and the
tissue.
Where the arc first
strikes, the tissue is coagulated.
The resistance of the
coagulated tissue goes up, so the arc moves to an adjoining area with less
resistance.
The process goes on
until the area is covered.
Perhaps like lightning not
striking twice in the same place.
The main problem with high
voltage is the increased risk of capacitive coupling: see below.
Presumably there is also a
risk of the arc deviating to some tissue or instrument that came within reach
causing inadvertent tissue damage.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Problems
with diathermy.
Problems with bipolar diathermy.
These are few and far
between.
The main ones will be
operator error: treating the wrong tissue.
Or allowing super-heated
tissue after treatment to come into contact with other tissue, such as bowel,
and inflict thermal damage.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Problems
with unipolar diathermy.
The same problems can occur
with open and laparoscopic surgery.
The risks are greater with
the latter.
The medium used to distend
the abdomen at laparoscopy must be non-combustible.
At hysteroscopy it should
be non-conductive if diathermy is to be used, so the electric current is not
dissipated.
Saline is conductive.
It can be used if the
diathermy is bipolar, such as Versapoint.
Pumping gas into the
abdomen means greater pressure is needed to ventilate the lungs.
The anaesthetist must be
aware of the problems.
There is a small risk of
cardiac arrest.
Pumping fluid into the
uterus creates the potential for fluid overload.
This will be related to:
the
pressure used,
the
duration of the procedure,
the
surface area of the uterine cavity
and
the extent of the damage to the endometrium.
This has been extensively
described after trans-urethral resection of the prostate TURP.
TURP syndrome is mainly due
to fluid overload, but some of the chemicals used, such as dextran have been
linked to direct toxic effects.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Direct
coupling.
This means that the active electrode comes into physical contact with something
it should not.
The whole of the active
electrode cannot be seen at the same time, especially at laparoscopy.
Thus an insulation failure
half way up the probe, allowing direct transfer of current from the probe to
adjacent tissue, would not be seen.
You would be looking at the
active tip of the instrument, not elsewhere.
You might not see direct
contact between the probe and another conductive instrument, e.g. the
laparoscope.
The insertion of multiple
instruments during laparoscopic surgery increases the risk.
When inadvertent damage has
occurred, it is usually not recognised during the surgery and the problem may
only manifest itself hours or days later.
This means that any
deviation from normal recovery should occasion thoughts of possible damage.
Good documentation is
essential if you are to keep out of court!
The increasing practice of
recording the surgery on video is to be commended.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Capacitive
coupling.
Below is a depiction of a capacitor.
There are two, circular,
conductive plates with a wire attached to each.
They are separated by a
gap.
This could be air or any
other material that is a resistor and does not let electricity pass.
The magical thing about a
capacitor is the ability of an alternating current in one side of the device to
induce an alternating current on the other side.
This occurs
without there being a physical connection between the two sides.
Electrons are negatively
charged.
Charged particles repel
those with the same charge.
It is like north and south
poles on a magnet attracting their opposites and repelling identical poles.
A negative electric field
will also repel electrons.
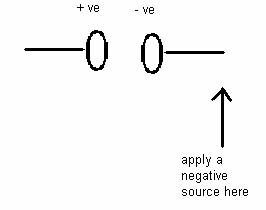
Imagine we apply a negative
field to the end of the wire attached to the right-hand plate.
Electrons would be driven
from the end of the wire towards the plate, where they would congregate.
As the electrons are
negatively charged, this would mean that the plate would become negatively
charged.
This would have an effect
on the electrons on the left-hand plate, driving them away.
Depleted of electrons, the
left-hand plate would become positively charged.
Take away the original
negative source and the electrons will move back to their starting positions.
Any movement of electrons
is an electric current.
So, the original
application of the negative source to the end of the wire attached to the
right-hand plate will make a current flow in the right-hand wire and plate.
And the charging of the
right hand plate will induce a current in the left-hand plate and wire.
Removal of the negative
source will cause reverse currents in both plates and wires.
Anything that makes an
alternating current in the right-hand wire and plate induces an alternating
current in the left-hand wire and plate.
I hope this makes sense.
In surgery, capacitive
coupling means that you have something acting as a capacitor.
A capacitor must have two
conductors separated by a resistor.
In the above example, it
was two metal plates separated by air.
The current flow must be
alternating.
In surgery you have the
wire leading to the active probe:needle-point, forceps or whatever.
The wire is surrounded by
an insulating sheath.
In turn, this is usually
surrounded by a metal cannula.
So we have a capacitor: the
same set-up as the example above, except it is radial, not linear.
This is meant to be a white bit representing the active wire.
With a brown bit around it representing the insulation
covering the wire
And an outer black layer representing the metal cannula.
The blue bits just helped me put the diagram together, so can
be ignored.
The fundamental point is:
a current flowing down the active wire
will induce a current in the metal cannula.
Alternative arrangements,
e.g. supplying the current via an operating laparoscope, will do the same.
The stray current
flowing in the cannula will try to return to the pad attached to the
thigh of the patient, just like the current from the probe itself.
It will travel via any
tissue with which it is in contact.
In most cases the amount of
current is too small to do damage.
In addition, it will
usually pass to the thigh pad via the abdominal wall where the cannula is in
contact and cause no harm.
This is because the contact is
over a large enough area.
But it could go via bowel or anywhere else.
The worst scenario is if the
metal cannula is insulated from the
abdominal wall, e.g. by a plastic insert.
The stray current
then cannot discharge via the abdominal wall, so will be more likely to travel
via bowel etc. and cause harm.
You might think that the
solution would be to use non-conductive cannulae.
This does not eliminate the
problem.
The body of the patient acts
as a conductor.
Once again you have a
capacitor.
The conducting electrode is
the probe and the wire leading to it.
The surrounding insulation and non-conductive cannula act as the
insulator.
The body can function as a conductor outside of that.
The surgeon could even be
the second conductor and get an electric shock.
The risk of capacitive
coupling increases with high voltages, so you will not be zapping away with
fulguration at laparoscopy.
The thinner the insulating
layer, the closer the two conductors and the bigger the induced current.
We are back to inverse
square laws, but they will not feature in the MRCOG.
Thin insulation can be a
design feature in a very slim instrument or occur with wear and tear.
It is reckoned that an
active electrode being passed through a metal irrigation/ suction device is
particularly dangerous.
Capacitive coupling occurs
every time an alternating current is applied to one of the conductors in a
capacitor.
So it happens every time
you use diathermy.
But
it is usually so small and so well dissipated via the contact between the
cannula and the abdominal wall that it causes no problem.
The problem is solved by
the newer diathermy machines which measure stray current and switch the
machine off if it is at a potentially harmful level.
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
Suggested
structure of a MRCOG viva.
I would include the following headings:
-
What is diathermy?
-
What kind of current is used and at what frequency?
-
Why use this kind of current?
-
What types of diathermy current are used?
-
How is diathermy applied?
-
What are the risks associated with
diathermy?
Write your answer, then e-mail it to me for my
version
go to the top of the page
go to the list of
contents
go to the bottom of the page and
other links
